Introduction
Acne vulgaris is a disease of the pilosebaceous unit (hair follicles and accompanying sebaceous glands), which is one of the most common and relapsing inflammatory skin disorders with a global burden of 9.4%.1 As adolescence approaches, acne is more prevalent in males than females, but also affects middle-aged adults, especially women.2 It presents a pleomorphic array of lesions, including comedones, papules, pustules, and nodules, typically affecting areas with highly sebaceous follicles, such as the face and central facial areas of the chest and back. The pathogenesis of acne is a multifactorial process involving multiple factors that contribute to its formation, including hyperactive sebaceous gland, comedogenics, follicular hyperkeratinization of the sebaceous glands duct, proliferation of Cutibacterium acnes, release of inflammatory mediators, excessive sebum production, and genetics.3 In addition, cosmetics, hair wax, hormones and oral contraceptives can also lead to formation of acne.4 Over the years, topical and systemic treatments are the first-line treatment of acne.5 However, pharmacological therapies have potential side effects and the development of antibiotic resistance which made it undesirable for patients.6 At present, cosmetological methods were reported in the treatment of acne such as cosmetic acids including (phytic, pyruvic, lactic and ferulic acids) combined with oxybrasion treatment, results were satisfactory; however, the study was conducted only on a group of women which has a lack of evidence of its efficacy on men as well.7 Recent guidelines suggest an earlier and appropriate treatment option for acne, which may decrease the chance of forming acne sequelae.8 Some patients after acne regression may develop clinically relevant sequelae that can have a serious psychological and social burden on patients’ life.9 These sequelae include acne scars (atrophic scars, hypertrophic scars, and keloids), post-acne pigmentation, and post-acne erythema. Aiming to prevent sequelae formation should, therefore, be the focus of acne treatment instead of just controlling acne. The most common sequela of inflammatory acne is post-acne erythema (PAE). It mainly affects light skin types. Despite the unknown pathogenesis, previous studies have suggested that PAE is associated with erythematous macules and telangiectasia. In contrast, telangiectasia results from changes in the microvascular system in the superficial dermis.10 These lesions may resolve slowly and spontaneously; however, in most patients, persistent post-acne erythema may last for years if no interventional management is conducted, which is cosmetically unacceptable and has great psychological, social, and financial implications for the patients.11 Some patients tend to cover up PAE using cosmetic products such as foundations, concealers, or any other cream products, but the results are not very satisfactory, as some of these products may contain sensitive substances that can worsen the appearance of PAE and cause side-effects in some patients. Various therapies have been proposed to manage this cosmetic problem, but with resistance to oral and topical therapies,10,12 and with no consistent results and minimal side-effects for laser and light-based devices.13–18
The IPL is a flashlamp-pumped light source that provides a non-coherent polychromatic source; it integrates with a range of wavelength bands, from 515 to 1200 nm, that can penetrate the skin from superficial to deeper vessels and has been used in the management of various conditions such as facial telangiectasia, photoaging, and inflammatory diseases such as rosacea and acne.19,20 IPL M22 Optima device (Lumenis, Yokneam, Israel) is one of the most widely used IPL machines for the treatment of photodamage and skin rejuvenation.21 The M22 has various filters that can be used according to skin condition, including novel dual-band filters with wavelengths of 530–650 nm and 900–1200 nm (vascular filter) and 400–600 nm and 800–1200 nm (acne filter), which have been used in the treatment of facial telangiectasia and acne vulgaris. However, although previous studies have shown that IPL had a positive effect on increasing the clearance rate of PAE and acne vulgaris, the effect of the IPL narrow-spectrum vascular filter should be further improved. Based on the aforementioned facts, the present study attempted to compare the therapeutic effect and safety of IPL narrow-spectrum vascular (530–650 nm and 900–1200 nm) filters and IPL broad-spectrum (560–1200 nm)/(590–1200 nm) filters for the treatment of post-acne erythema lesions and the control of acne relapse. This study included a blank control group to exclude factors that could have contributed to PAE disappearance spontaneously.
Materials and Methods
Subjects
Sixty patients diagnosed with PAE at the Department of Dermatology of the First Affiliated Hospital of Nanchang University between May 2021 and January 2022, aged 17–42 (mean age: 25.95 years) (9 males, 51 females) were enrolled in this study. Written informed consent was obtained from each of the participants before study enrollment. The exclusion criteria were as follows: patients with hypersensitivity to visible light, patients with skin inflammatory lesions and open wounds, patients with a history of sun exposure within 1 month, patients used pills like yeast tablets, sulfur tablets, photosensitizing herbs, pregnant and lactating women, patients who had done facial fillers or botulinum toxin therapy within 3 months prior to the treatment, patients who had undergone any laser or light treatments.
Patients with a history of skin cancer, prior acne therapy including isotretinoin therapy within 6 months, chemical peeling, or refusal to sign consent were excluded from this study. Patients who met the inclusion criteria were randomly divided into three groups: the first group (n=20, male/female ratio = 2/18, age range = 17–33, mean age = 26) received IPL narrow-spectrum vascular (530–650 nm and 900–1200 nm) treatment, and the second group (n=20, male/female ratio = 4/16, age range = 17–42, mean age = 27.2) received IPL broad-spectrum 560 nm/590 nm treatment. The blank control group (n=20, male/female ratio = 3/17, age range = 19–34, mean age = 25 years) did not receive any specific treatments. The demographic characteristics of patients in each group are presented in (Table 1).
 |
Table 1 The Demographic Characteristics of Patients in Each Group |
Treatment Procedure
An intense pulsed light device (M22; Lumenis Limited) was integrated with a sapphire Chill Tip system for epidermal cooling with a wavelength of 515–1200 nm. Three wavelength bands were configured (530–650 nm and 900–1200 nm), (560–1200 nm), and (590–1200 nm). The following parameters were adjusted for each filter. Vascular filter (530–650 nm and 900–1200 nm), (fluence = 20–22 J/cm2, pulse duration = 4.0–6.0 ms, pulse delay = 20–30 ms), 560–1200 nm (fluence = 17–19 J/cm2, pulse duration = 3 ms, pulse delay = 20–30 ms), and 590–1200 nm (fluence = 17–19 J/cm2, pulse duration = 3.5 ms, pulse delay = 30–40 ms). Each patient in the IPL treatment group received four sessions with an interval of 4 weeks. The treatment was delivered in two passes over the red macules. No topical aesthetic was administered before treatment. The post-treatment regimen involved application of ice pack for 20 minutes to reduce burning sensation and medical mask for 15 minutes to enhance facial hydration immediately after the treatment. Ask the patients to apply SPF of 50 sunscreen every morning until clinical follow-up, avoidance of daily cosmetics products containing irritating ingredients, mineral oils, cleansers with fragrances and makeup for at least 48 hours after each treatment.
Efficacy Assessment
Primary Outcomes
The severity of PAE before and after the treatment was scored and graded by a dermatologist who did not participate in IPL treatment based on CAT (CEA, Area, Telangiectasia) scale.22 The total CAT score = CEA×Area+Telangiectasia. The clinical improvement of PAE was determined using the Investigators Global Assessment (IGA) four-point grading scale: poor (<25%), fair (25–50%), marked (51–75%), and excellent (>75%) improvement. The improvement score index for each patient was calculated by the following formula: (The total score before the treatment ‒ The total score after the treatment)/The total score before the treatment×100%.23 After obtaining informed consent, each patient was asked to complete the CHINESE CADI (Cardiff Acne Disability Index) (translated) questionnaire with a total of five questions, and the scores for all five questions range from 0 to 15 (score for each question = 0–3). Erythema-induced QoL impairment by CADI scores was graded as no impairment (CADI=0), mild impairment (CADI=1–5), moderate impairment (CADI=6–10), or severe impairment (CADI=11–15).24
Secondary Outcomes
The patients in the three groups were followed up 4 months after the total treatment ended, and the recurrence rates of erythema and acne were observed and calculated. After each IPL treatment, adverse reactions including blisters, pigmentation, and erythema were counted and recorded for each group. Four months later, at follow-up, patients were asked to assess the therapeutic effect using a (0–4) point scale: highly satisfied, 4 points; very satisfied, 3 points; satisfied, 2 points; neutral, 1 point; and not satisfied, 0 points. Total satisfaction rate = (highly satisfied + very satisfied + satisfied) / total number of patients × 100.
Statistical Analysis
The data were preliminarily sorted using Excel 2010 and expressed as “mean ±standard deviation”, and the non-normal distribution was expressed as median and quartile interval M (P25–P75). One-way ANOVA was used to compare the normal distribution between the two groups, the paired t-test was used to compare the mean difference before and after the treatment, and the non-parametric test was used to compare the two groups with non-normal distribution-values of less than 0.05 were considered statistically significant.
Results
CAT (CEA, Area, Telangiectasia)
- CEA: After the treatment there was a significant difference between the three groups (H=27.677, P<0.05) (Table 2), CEA score of the IPL vascular group was significantly lower than that in the 560 nm/590 nm and the blank control groups (P<0.05) (Figure 1A).
- Area: The area score of the IPL vascular group was significantly lower than that of the blank control and 560 nm/590 nm groups after treatment (Figure 1B) (Table 3), and the area score of the IPL vascular group after treatment was significantly lower than that before treatment (P=0.002).
- Telangiectasia: Three-Point Telangiectasia score: The telangiectasia score in all patients was 0, as all patients in the three groups presented with no telangiectasia.
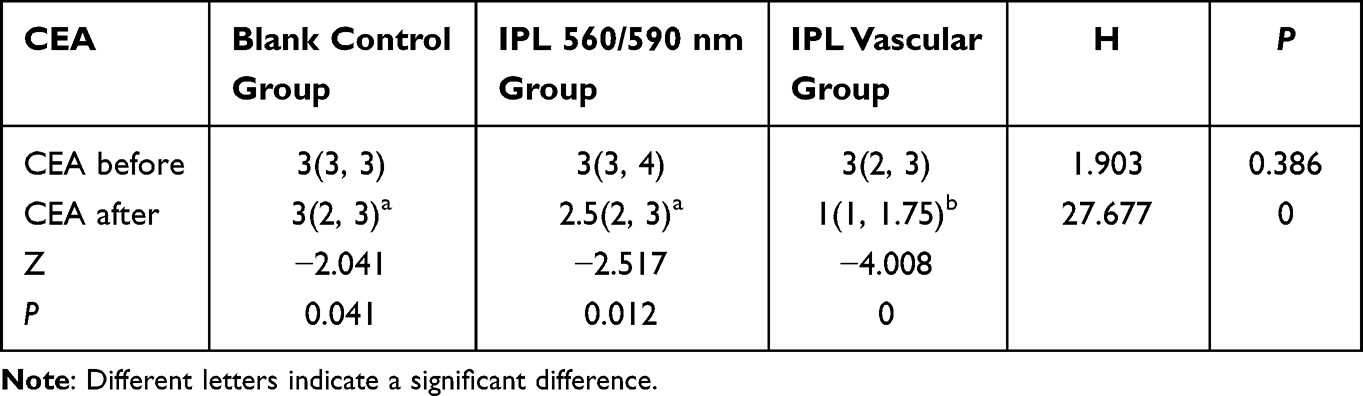 |
Table 2 The Comparison of CEA Score Between the Three Groups Before and After the Treatment |
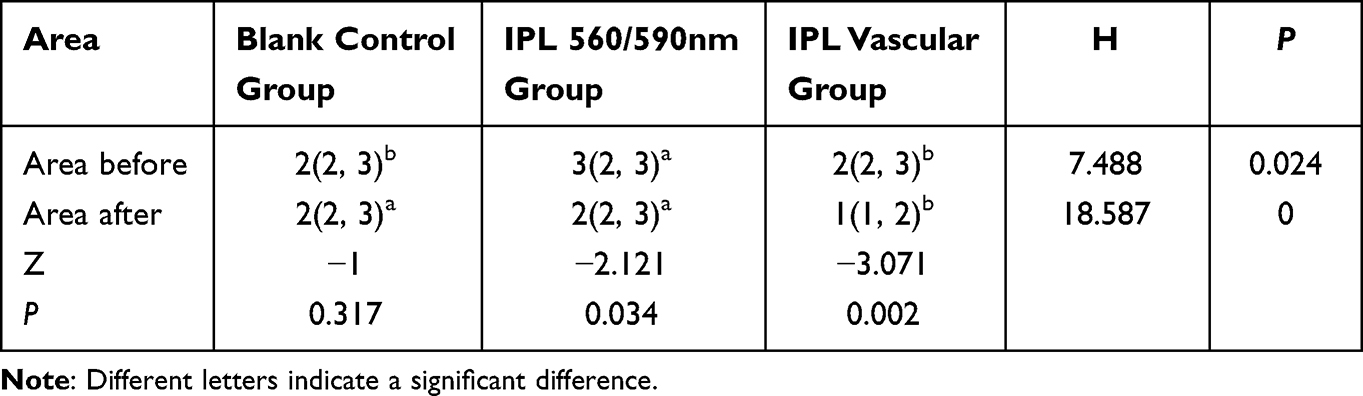 |
Table 3 The Comparison of Area Score Between the Three Groups Before and After the Treatment |
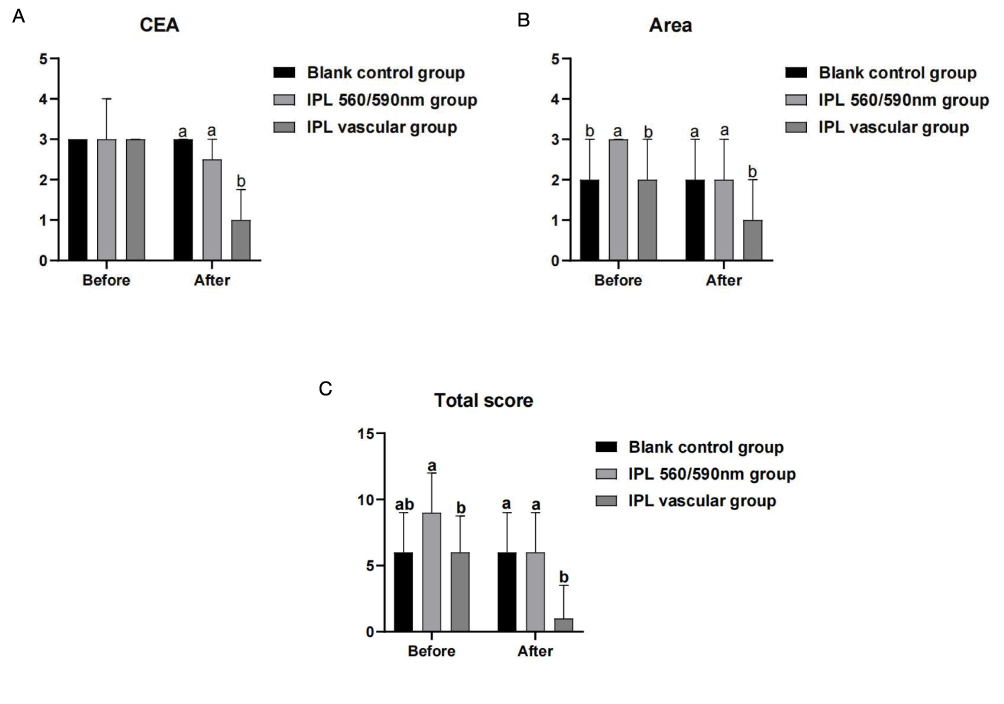 |
Figure 1 (A) The comparison of CEA score between the three groups before and after the treatment. (B) The comparison of Area score between the three groups before and after the treatment. (C) The comparison of total score between the three groups before and after the treatment. Note: Different letters indicate a significant difference. |
Total score: Before treatment, the total score of the 560/590 nm group was significantly higher than that of the IPL vascular group and the blank control group, while after the treatment the total score of the IPL vascular group was significantly lower than that of the blank group and 560 nm/590 nm group (P<0.05) (Figure 1C). Significant differences were observed between the IPL vascular groups before and after treatment (Table 4). The results showed that clearance of the PAE after IPL vascular treatment resulted in better results.
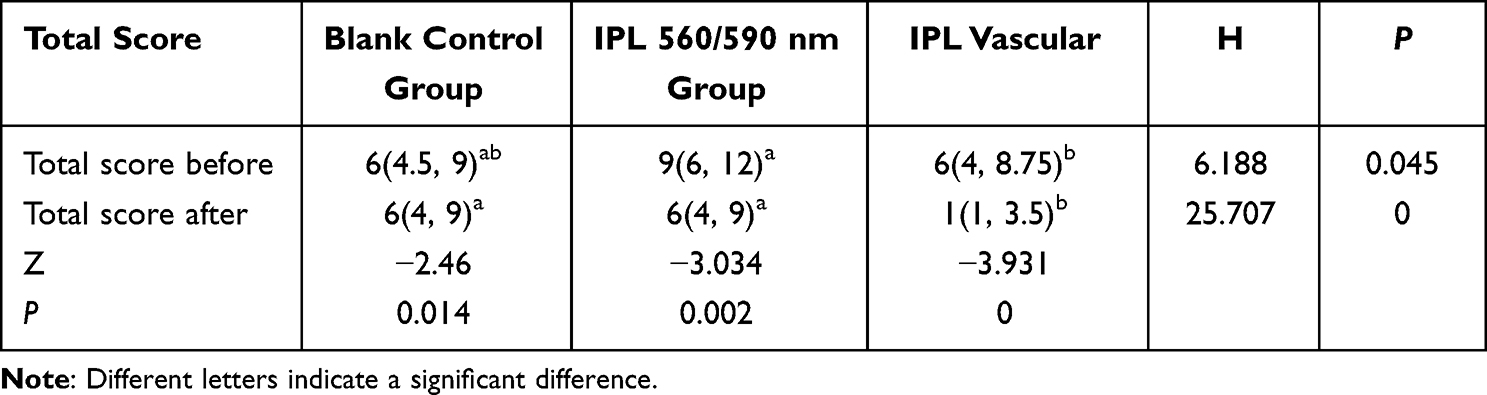 |
Table 4 The Comparison of Total Score Between the Three Groups Before and After the Treatment |
Investigators Global Assessment (IGA)
There was a significant difference in PAE improvement rate between IPL vascular group and IPL 560/590 nm group, PAE improvement rate in IPL vascular group was significantly higher than that in the blank control group, and there was no significant difference between IPL 560 nm/590 nm group and blank group (Figures 2–4; Table 5). The improvement rate of PAE in the IPL vascular group was higher than that in the other two groups (Figure 5).
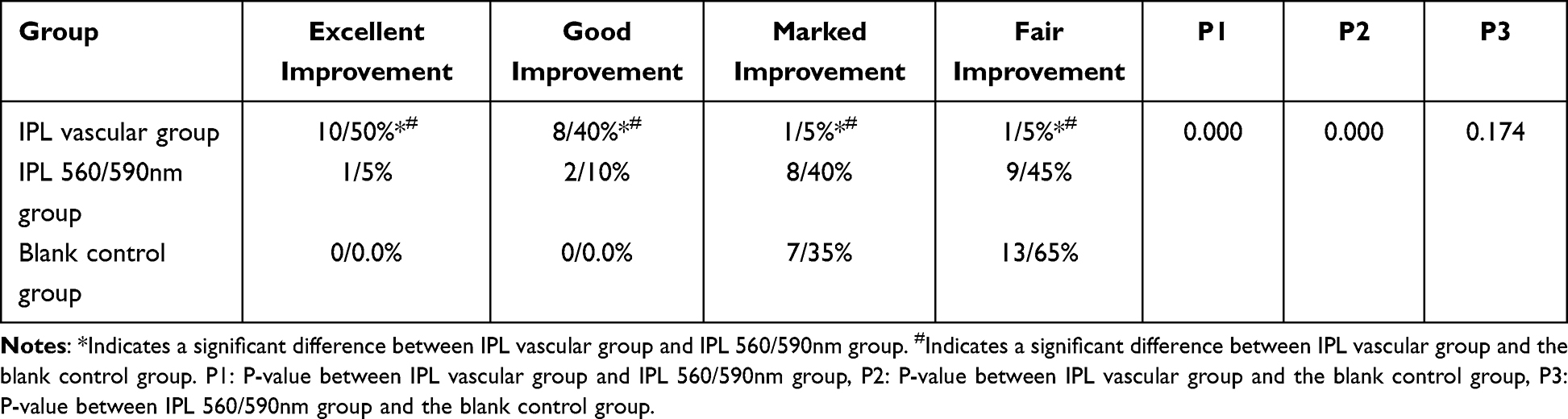 |
Table 5 The Comparison of Improvement Degree Between the Three Groups |
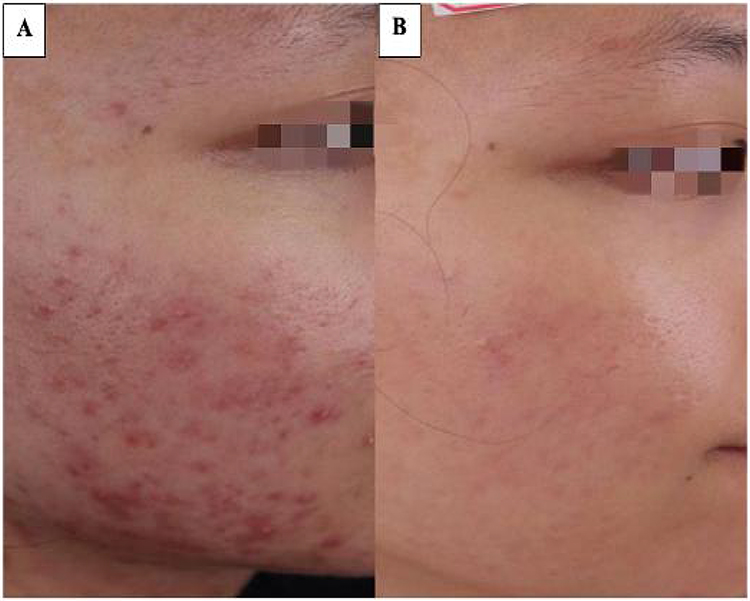 |
Figure 2 A 25-year-old female with PAE in the IPL vascular group: (A) before the treatment, (B) 1 month after the total treatment has finished, showing an excellent improvement in PAE (>75%). |
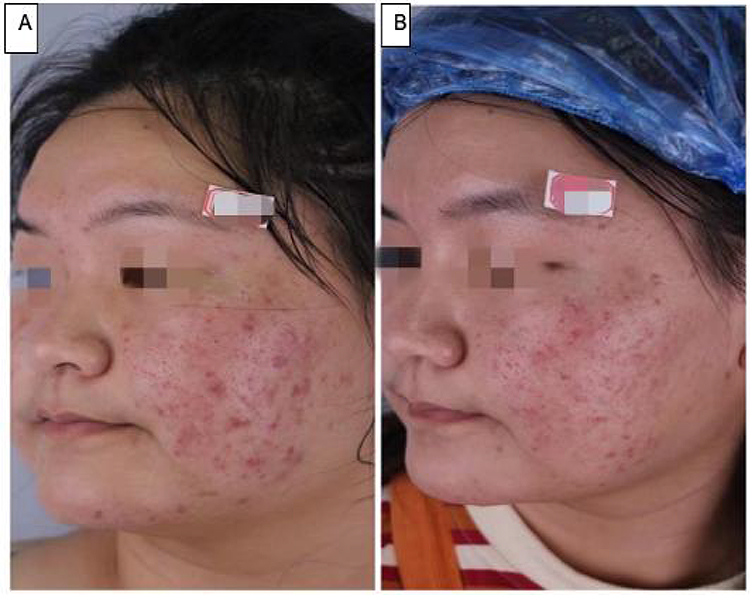 |
Figure 3 A 20-year-old female with PAE in the IPL 560/590 nm group: (A) before the treatment, (B) 1 month after the total treatment has finished, showing poor improvement in PAE (<25%). |
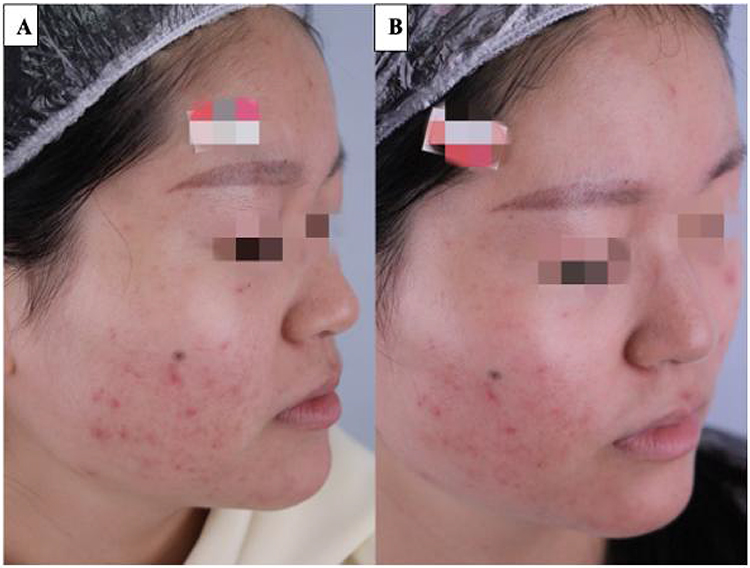 |
Figure 4 A 24-year-old female with PAE in the blank control group: (A) months before the follow-up, (B) at the follow-up, showing no improvement in PAE. |
 |
Figure 5 The comparison of improvement degree between the three groups. |
Cardiff Acne Disability Index (CADI)
The CADI score was used to evaluate the impact of PAE on Quality of Life. The CADI score in the IPL vascular group was significantly lower than that in the IPL 560 nm/590 nm and blank control groups (Table 6). There was no difference in the CADI score between the IPL 560 nm/590 nm group and blank control group after treatment (Figure 6). There were significant differences between the IPL vascular group before and after the treatment (P<0.05).
 |
Table 6 The Comparison of CADI Score Between the Three Groups Before and After the Treatment |
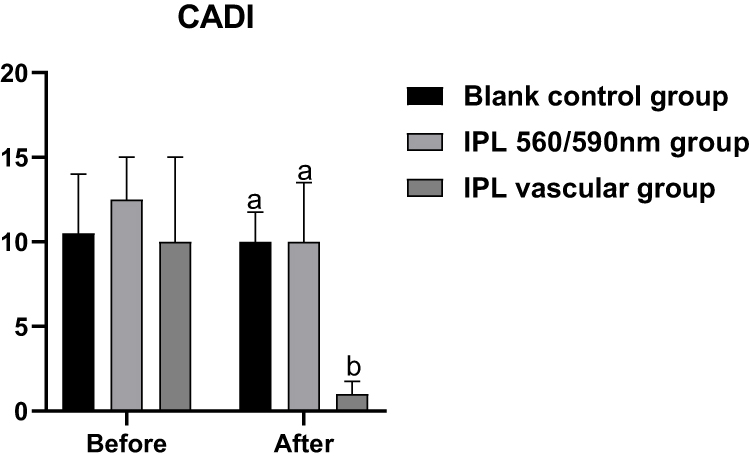 |
Figure 6 The comparison of CADI score between the three groups before and after the treatment. Note: Different letters indicate a significant difference. |
Patient Satisfaction
One month after the total treatment was completed, patients were asked to assess the results by referring to baseline photographs, and the results showed that the total satisfaction rates in the IPL vascular group, IPL 560/590 nm group, and the blank control group were about 95%, 40%, and 10%, respectively. Patient satisfaction in the IPL vascular group was significantly higher than that in the control group (P<0.05) (Table 7). According to our results, the satisfaction rate of the IPL vascular group was higher than that of the other two groups (Figure 7).
 |
Table 7 The Comparison of Patient’s Self-Satisfaction Between the Three Groups After the Treatment |
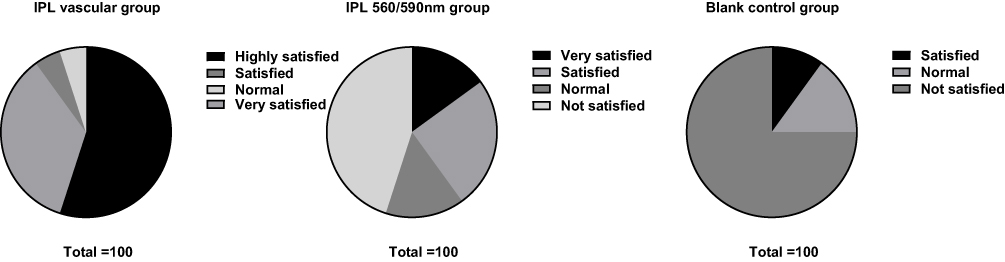 |
Figure 7 The comparison of patient’s self-satisfaction between the three groups after the treatment. |
Adverse Effects and Relapse
All patients tolerated the pain during the treatment, and after the last treatment, the patients in the three groups were followed-up: acne recurrence rate of the IPL vascular group, IPL 560/590 nm group, and the blank control group (0%, 40%, 15%, respectively) (Figures 8 and 9). There was a significant difference among the three groups (X2, 10.909, and 0.004) (Table 8). Flushing was observed in all patients in the IPL treatment groups. After the IPL 590 nm cut-off filter treatment, two patients (10%) had pigmentation that disappeared at follow-up, and three patients (15%) had blisters that lasted for 4 days after treatment.
 |
Table 8 The Comparison of Acne Recurrence Between the Three Groups After the Treatment |
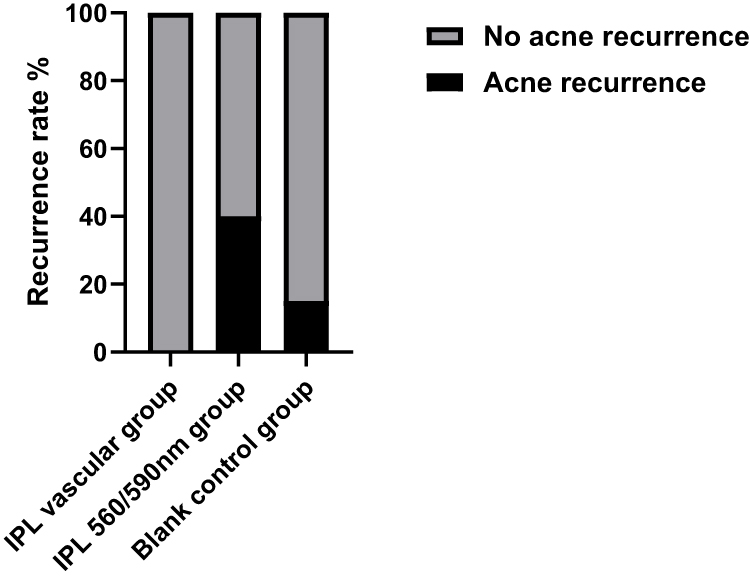 |
Figure 8 The comparison of acne recurrence between the three groups 4 months after the last session. |
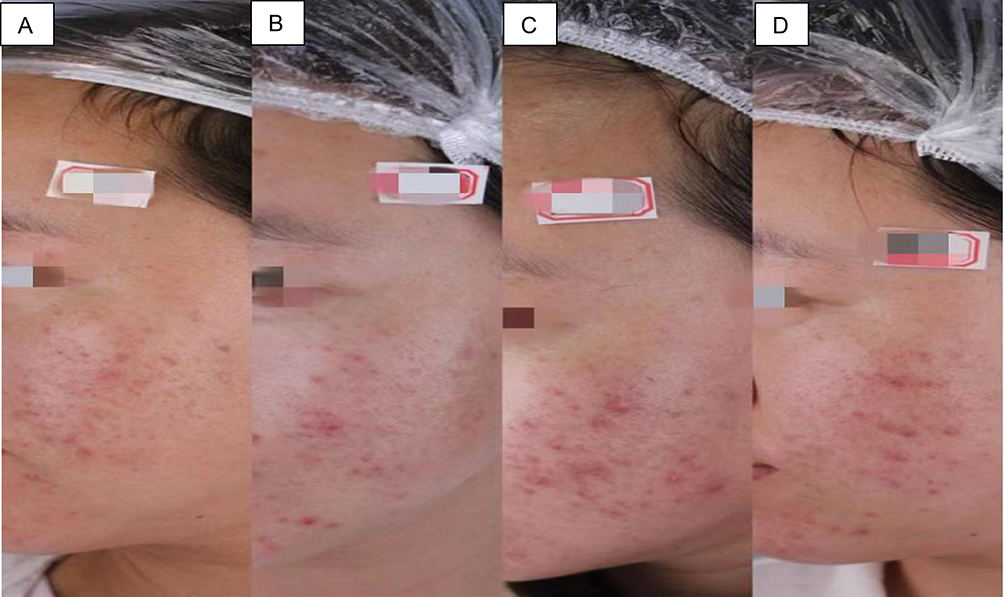 |
Figure 9 A 30-year-old female showing acne recurrence following IPL 590 nm treatment: (A) Before 590 nm treatment; (B) after the first session of IPL 590 nm; (C) after the second session of 590 nm treatment, and (D) at the follow-up. |
Discussion
Acne vulgaris affects nearly 80% of adolescents and young adults,25 and it is the eighth most prevalent disease worldwide.26 After the clearing process of inflammatory acne, usually persistent sequelae such as post-acne erythema, post-inflammatory hyperpigmentation, and scarring induced by inflamed acne may develop.27 Post-acne erythema (PAE) is the most common sequelae of acne inflammation, which is aesthetically undesirable and associated with a psychological impact on patients.13,14 PAE consists of telangiectasia and erythematous lesions located in the very superficial dermis that remain after inflammatory acne resolves.18
Although it has been shown to predict long-term treatment outcomes, little is known about how patients perceive this condition and its impact on their self-image. The primary goals of post-acne erythema treatment are to control and treat existing lesions, prevent acne relapse, and improve quality of life. At present, a variety of studies have been proposed to deal with this cosmetic problem, but the results are inconsistent and accompanied by a series of side-effects, including topical therapies including brimonidine, vitamin C, and tranexamic acid, which are used in the management of PAE. However, the long period of treatment, less effective results, and adverse reactions such as erythema, pruritus, and dryness make it clinically not the main standard treatment.28,29 When oral and topical therapies cannot achieve satisfactory results, investigating a new treatment plan is often encountered by clinicians. As laser- and light-based devices may provide faster responses and fewer treatment sessions, they have become a treatment option for patients with PAE. Up to the present time, there have been a few studies on the therapeutic effects of light-based technology for PAE such as Intense pulsed light (IPL),14 fractional micro-needling,18 and pulsed dye laser (PDL).27 When choosing light based modality in the treatment of PAE or any photo-damaged skin conditions, the clinicians should consider multiple variables to achieve a satisfactory result for the patients such as an appropriate wavelength band that can effectively target hemoglobin or small blood vessels, how to reduce the probability of acne recurrence, how to reduce the risk of epidermal hypopigmentation and pigmentation, and finally provide better treatment effects for patients. Intense pulsed light (IPL) has been shown to be one of the most effective treatments in PAE, as it emits a broad spectrum of light between 515 and 1200 nm that can be modified by cut-off filters to target specific chromophores (hemoglobin, melanin, and water) to varying degrees without significant damage to the surrounding tissue. Based on the concept of selective photo thermolysis the primary hemoglobin protein absorption peaks are at 418, 542, and 577 nm.30 The range of the secondary hemoglobin absorption peak is 800–1200 nm, that can specifically target the blood vessels located deep in the skin.31 Many studies reported the successful use of M22 devices in the treatment of photodamaged skin and skin rejuvenation.32 In our study, we compared the efficacy and safety of IPL narrow-spectrum vascular (530–650 nm and 900–1200 nm) filters and IPL broad-spectrum (560–1200 nm or 590~1200 nm) filters in the treatment of PAE. Our results showed that M22 IPL narrow spectrum Vascular (530–650 nm and 900–1200 nm) filters are more effective in the clearance of PAE; to the best of our knowledge, this is the first prospective comparative study to evaluate the efficacy and safety between IPL narrow and broad spectrum filters in the treatment of PAE. We conducted the current study to determine whether IPL narrow spectrum vascular filters can improve PAE related to inflammatory acne.33 IPL vascular (530–650 nm) wavelengths retain the primary hemoglobin protein absorbance spectrum and reduce the absorbance from melanoma and target blood vessels in the superficial dermis; IPL vascular (900–1200 nm) wavelengths include the secondary absorbance spectrum of hemoglobin protein which damages blood vessels located in the deep dermis. In this study, we used IPL vascular (530–650 nm and 900–1200 nm) with 20–22 J/cm2 energy, and after four sessions with an interval of 1 month. Patients showed an overall improvement of approximately 95% without any adverse effects, such as hyperpigmentation, blisters, or acne relapse. Bjerring et al34 conducted a study of 35 patients with vascular lesions and a reduction in erythema by fair to excellent clearance was obtained in 72.7% of patients treated with the IPL narrow wavelength band (530–750) nm. Tsunoda et al31 showed the efficacy of an IPL narrow-band (500–635 nm) in reducing redness in a case series of three patients with diffuse erythema without damage to the surrounding tissue. Chang et al35 evaluated an IPL device (530–750 nm, 7.5–8.0 J/cm2) in 30 Korean females with inflammatory acne associated with PIE. After three sessions in 3 weeks, red macules, irregular pigmentation, and skin tone improved in 63% of the patients.
Schroeter et al36 demonstrated a study on the treatment of erythema and vascular components in 60 patients, 75–87% clearance was achieved using a 550 nm cut-off filter with an average of 4.1 treatments. Kassir et al37 reported improvement in facial redness in 80% of patients with rosacea, and 78% of patients showed a reduction in flushing and improvement in skin texture using an IPL 530 nm filter with no adverse effects in any patient. Gao et al23 in a retrospective study of 160 patients with facial telangiectasia, compared pulsed dye laser with IPL vascular filter, and the results showed significantly better indices of lesion severity and improvement scores of facial telangiectasia after IPL vascular treatment. Chen et al38 reported a study of IPL 560 nm/590 nm combined with IPL 420 nm for PAE treatment. The results showed that the improvement rate of PAE was approximately 81.8%. In our study, IPL 560–1200 nm and 590–1200 nm cut-off filters were selected according to the patient’s skin colour, confirming that IPL 560–1200 nm/590–1200 nm had a certain effect on PAE. Our study included 60 patients with PAE and evaluated the changes in PAE before and after treatment. Regarding the CAT score and in comparison, with the blank control group, we further confirmed the effect of IPL vascular group and IPL 560/590 nm group on PAE treatment. The CADI score in the IPL vascular group showed a significant decrease compared to the other two groups (P<0.05%), which explains the role of IPL vascular treatment in the improvement of Quality of Life. Following IPL 560/590 nm treatment, redness was observed in all patients after the treatment, two patients had pigmentation, and three patients had blisters for 4 days after the treatment session. In the IPL vascular group, only flushing was observed in five patients as an adverse effect. The degree of patient satisfaction in the IPL vascular group was higher than that in the other two groups (P<0.05), which showed that the efficacy of IPL vascular treatment was superior to that of the IPL 560/590 nm group and blank control group. Previous studies have shown that light‐energy‐based devices have been used for the treatment of inflammatory acne, and that each device has therapeutic advantages and disadvantages.
Vascular lasers such as 595-nm PDL are effective for the treatment of inflammatory and non-inflammatory acne, but with a risk of acne flare-up and are less safe in dark-skin patients.39,40 A 532 nm KTP has a poor penetration rate of different structures in the skin, such as sebaceous glands and blood vessels, so it is easy to cause scars.41 The mechanism of IPL in the treatment of acne vulgaris can be explained as inactivating Propionibacterium acne, inhibiting sebaceous gland secretion through photothermal action, and thermal damage to the blood vessels with a small diameter that supplies sebaceous glands, to achieve the purpose of reducing inflammation.42 Although the therapeutic effect of IPL on acne vulgaris has been established, the characteristics of different wavelength bands need to be further analysed and clarified in order to improve the efficacy of IPL.19 Our study also conducted a statistical analysis of the acne recurrence rate in each group. Eight (40%) out of 20 patients in the IPL 560/590 nm group and three (15%) in the blank control group had acne recurrence, while no acne recurrence was found in the IPL vascular group, consistent with the results of Wu et al,11 who reported acne relapsing in seven patients (11.7%) treated with IPL 560–1200 nm and 590–1200 nm cut-off filters after 3–7 sessions at intervals of 4 weeks, Monib et al,43 who showed three out of 15 patients treated with IPL 400 nm filter showed acne exacerbation after the first (−60%, −28.6%, −6.1%) and second (−35%, 47.6%, 36.4%) sessions, respectively, and Ross et al,33 who used IPL (525–1200 nm) in the treatment of acne; after four sessions and 2 week intervals, the patient showed acne relapse (3–8 weeks) at follow-up. The energy of IPL broad-spectrum filters may affect larger and deeper tissues.44 This may lead to non-selective diffusion of energy in the dermis and eventually lead to adverse reactions, such as acne recurrence and pigmentation, which are more likely to occur in patients with skin type IV.
The destructive effect of the IPL vascular filter is characterized by oxyhaemoglobin and deoxyhaemoglobin, which can destroy small, dilated blood vessels in PAE lesions and prevent acne relapse. The vascular filter decreases the amount of light absorbed by melanin pigments by excluding the emission of light at wavelengths of 650–900 nm. Such exclusion of these wavelengths reduces the risk of overheating the epidermis and increases the amount of light absorbed by haemoglobin.45
Theoretically, chemical reactions directly depend on temperature. The higher the temperature, the faster a given chemical reaction will proceed to destroy the P. acnes.46,47 IPL vascular filters can convert the light absorbed by haemoglobin into heat energy, which raises the temperature of central blood vessels by 80–90°C, causing thrombosis in the superficial blood vessels and increasing the rate of chemical reaction.48 Acne produces and stores large amounts of porphyrins in the metabolic process. Therefore, once porphyrins produced by P. acnes are exposed to IPL vascular 530–600 nm wavelength, they become chemically activated and form reactive oxygen species capable of destroying P. acnes and produce an anti-inflammatory reaction.49
The second band (900–1200 nm) targets the sebaceous glands directly and penetrates deeper into the skin.50,51 Previous studies have confirmed the therapeutic effect of the M22 IPL acne filter on acne vulgaris.41 In our investigation, after four sessions of PAE treatment using IPL narrow spectrum vascular (530–650 nm and 900–1200 nm) filters, an improvement rate of PAE lesions was about 95%. Based on previous literature and our clinical observations, we hypothesized that the use of the M22 IPL vascular filter in the treatment of PAE can effectively prevent acne recurrence. We believe that IPL vascular filters can be considered an alternative treatment for PAE as they can effectively treat PAE, reduce the recurrence of acne, and shorten the time and frequency of treatment. One limitation of the study was the small sample size. Further controlled prospective observations in larger sample size would be helpful to prove the effect of IPL narrow spectrum with higher level of evidence.
Conclusion
To the best of our knowledge, this is the first prospective analysis of an effective treatment of PAE using an IPL narrow-spectrum vascular filter. IPL narrow spectrum vascular (530–650 nm and 900–1200 nm) filters could be effective in reducing PAE severity and improving QoL; additionally, they have no adverse effects and control the recurrence of acne. However, further research into the mechanism underlying the action of this narrow wavelength band, as well as a comparative study of novel IPL dual-band filters, is recommended.
Abbreviations
PAE, post-acne erythema; IPL, intense pulsed light; P. acnes, Propionibacterium acnes; CAT, CEA, Area, Telangiectasia; CEA, clinical erythema assessment; IGA, investigator’s global assessment; CADI, Cardiff Acne Disability Index; PDL, pulsed dye laser; QoL, quality of life.
Ethical Approval
This study was approved by the Ethics Committee of the First Affiliated Hospital of Nanchang University. [2023]No.076. The procedures used in this study adhered to tenets of the Declaration of Helsinki.
Informed Consent
All the participants who appear in the figures contained in our manuscript provided informed consent for their images to be published.
Acknowledgments
The authors would like to acknowledge the laser department residents and nurses for their assistance with this study.
Funding
This study was funded by the Health Commission of Jiangxi Province, China [grant number 202310288].
Disclosure
The authors declare no competing interests.
References
1. Ferlay J, Colombet M, Soerjomataram I, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int J Cancer. 2019;144(8):1941–1953. doi:10.1002/ijc.31937
2. Skroza N, Tolino E, Mambrin A, et al. Adult acne versus adolescent acne: a retrospective study of 1167 patients. J Clin Aesthet Dermatol. 2018;11(1):21–25.
3. Toyoda M, Morohashi M. Pathogenesis of acne. Med Electron Microsc. 2001;34(1):29–40. doi:10.1007/s007950100002
4. Dréno B, Bettoli V, Araviiskaia E, Sanchez Viera M, Bouloc A. The influence of exposome on acne. J Eur Acad Dermatol Venereol. 2018;32(5):812–819. doi:10.1111/jdv.14820
5. Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945–973. doi:10.1016/j.jaad.2015.12.037
6. Canavan TN, Chen E, Elewski BE. Optimizing non-antibiotic treatments for patients with acne: a review. Dermatol Ther. 2016;6(4):555–578. doi:10.1007/s13555-016-0138-1
7. Chilicka K, Rusztowicz M, Rogowska AM, Szyguła R, Nowicka D. Efficacy of oxybrasion and cosmetic acids on selected skin parameters in the treatment with acne vulgaris. Clin Cosmet Investig Dermatol. 2023;16:1309–1317. doi:10.2147/CCID.S407976
8. Tan J, Tanghetti E, Baldwin H, Stein Gold L, Lain E. The role of topical retinoids in prevention and treatment of atrophic acne scarring: understanding the importance of early effective treatment. J Drugs Dermatol. 2019;18(3):255–260.
9. Dréno B. Treatment of adult female acne: a new challenge. J Eur Acad Dermatol Venereol. 2015;29(S5):14–19. doi:10.1111/jdv.13188
10. Agamia N, Essawy M, Kassem A. Successful treatment of the face post acne erythema using a topically applied selective alpha 1-Adrenergic receptor agonist, oxymetazoline 1.5%, a controlled left to right face comparative trial. J Dermatolog Treat. 2022;33(2):904–909. doi:10.1080/09546634.2020.1789045
11. Wu X, Wang X, Wu X, et al. Intense pulsed light therapy improves acne-induced post-inflammatory erythema and hyperpigmentation: a retrospective study in Chinese patients. Dermatol Ther. 2022;12(5):1147–1156. doi:10.1007/s13555-022-00719-9
12. Genedy RM. Topical brimonidine tartrate as a novel treatment for facial erythema of rosacea and acne erythema. J Egypt Womens Dermatologic Soc. 2016;13(2):55–64. doi:10.1097/01.EWX.0000483162.96767.73
13. Kalantari Y, Dadkhahfar S, Etesami I. Post-acne erythema treatment: a systematic review of the literature. J Cosmet Dermatol. 2022;21(4):1379–1392. doi:10.1111/jocd.14804
14. Mathew ML, Karthik R, Mallikarjun M, Bhute S, Varghese A. Intense pulsed light therapy for acne-induced post-inflammatory erythema. Indian Dermatol Online J. 2018;9(3):159–164. doi:10.4103/idoj.IDOJ_306_17
15. Yoon HJ, Lee DH, Ok Kim S, Chan Park K, Woong Youn S. Acne erythema improvement by long‐pulsed 595‐nm pulsed‐dye laser treatment: a pilot study. J Dermatolog Treat. 2008;19(1):38–44. doi:10.1080/09546630701646164
16. Panchaprateep R, Munavalli G. Low-fluence 585 nm Q-switched Nd:YAG laser: a novel laser treatment for post-acne erythema. Lasers Surg Med. 2015;47(2):148–155. doi:10.1002/lsm.22321
17. Park KY, Ko EJ, Seo SJ, Hong CK. Comparison of fractional, nonablative, 1550-nm laser and 595-nm pulsed dye laser for the treatment of facial erythema resulting from acne: a split-face, evaluator-blinded, randomized pilot study. J Cosmet Laser Ther. 2014;16(3):120–123. doi:10.3109/14764172.2013.854626
18. Min S, Park S, Yoon J, Kwon H, Suh D. Fractional microneedling radiofrequency treatment for acne-related post-inflammatory erythema. Acta Derm Venereo. 2016;96(1):87–91. doi:10.2340/00015555-2164
19. Bennardo L, Patruno C, Zappia E, et al. Combination of specific vascular lasers and vascular intense pulsed light improves facial telangiectasias and redness. Medicina. 2022;58(5):651. doi:10.3390/medicina58050651
20. Kim BY, Moon HR, Ryu HJ. Comparative efficacy of short-pulsed intense pulsed light and pulsed dye laser to treat rosacea. J Cosmet Laser Ther. 2019;21(5):291–296. doi:10.1080/14764172.2018.1528371
21. Seo JK, Shin EJ, Jeong KH, Shin M. Clinician severity assessment grading scale on erythematotelangiectatic rosacea. Indian J Dermatol. 2021;66(2):203. doi:10.4103/ijd.IJD_611_19
22. Motley RJ, Finlay AY. Practical use of a disability index in the routine management of acne. Clin Exp Dermatol. 1992;17(1):1–3. doi:10.1111/j.1365-2230.1992.tb02521.x
23. Gao L, Gao N, Song W, et al. A retrospective study on efficacy of pulsed dye laser and intense pulsed light for the treatment of facial telangiectasia. J Drugs Dermatol. 2017;16(11):1112–1116.
24. Goodman G. Acne--natural history, facts and myths. Aust Fam Physician. 2006;35(8):613–616.
25. Hay RJ, Johns NE, Williams HC, et al. The global burden of skin disease in 2010: an analysis of the prevalence and impact of skin conditions. J Invest Dermatol. 2014;134(6):1527–1534. doi:10.1038/jid.2013.446
26. Layton AM, Thiboutot D, Tan J. Reviewing the global burden of acne: how could we improve care to reduce the burden?. Br J Dermatol. 2021;184(2):219–225. doi:10.1111/bjd.19477
27. Bae-Harboe YSC, Graber EM. Easy as PIE (postinflammatory erythema). J Clin Aesthet Dermatol. 2013;6(9):46–47.
28. Johnson AW, Johnson SM. The role of topical brimonidine tartrate gel as a novel therapeutic option for persistent facial erythema associated with Rosacea. Dermatol Ther. 2015;5(3):171–181. doi:10.1007/s13555-015-0078-1
29. Kurokawa I, Yoshioka M, Ito S. Split‐face comparative clinical trial using glyceryl‐octyl‐ascorbic acid/ascorbyl 2‐phosphate 6‐palmitate/DL‐α‐tocopherol phosphate complex treatment for postinflammatory hyperpigmentation, postinflammatory erythema and atrophic scar in acne vulgaris. J Dermatol. 2019;46(10). doi:10.1111/1346-8138.14930
30. Anderson RR, Parrish JA. Selective photothermolysis: precise microsurgery by selective absorption of pulsed radiation. Science. 1983;220(4596):524–527. doi:10.1126/science.6836297
31. Tsunoda K, Takahashi K, Ogino N, Yoshida A, Akasaka T. Treatment of facial telangiectasia with a small spot of intense pulsed light: a case series of three patients. J Dermatol. 2014;41(7):638–641. doi:10.1111/1346-8138.12517
32. Ping C, Xueliang D, Yongxuan L, et al. A retrospective study on the clinical efficacy of the intense pulsed light source for photodamage and skin rejuvenation. J Cosmet Laser Ther. 2016;18(4):217–224. doi:10.3109/14764172.2015.1114649
33. Tirico MC, Jensen D, Green C, Ross EV. Short pulse intense pulsed light versus pulsed dye laser for the treatment of facial redness. J Cosmet Laser Ther. 2020;22(2):60–64. doi:10.1080/14764172.2020.1717540
34. Bjerring P, Christiansen K, Troilius A, Dierickx C. Facial photo rejuvenation using two different intense pulsed light (IPL) wavelength bands. Lasers Surg Med. 2004;34(2):120–126. doi:10.1002/lsm.20000
35. Chang SE, Ahn SJ, Rhee DY, Choi JH, Moon KC, Suh HS. Treatment of facial acne papules and pustules in Korean patients using an intense pulsed light device equipped with a 530- to 750-nm filter. Dermatol Surg. 2007;33(6):676–679. doi:10.1111/j.1524-4725.2007.33142.x
36. Schroeter CA, Haaf-von Below S, Neumann HAM. Effective treatment of rosacea using intense pulsed light systems. Dermatol Surg. 2006;31(10):1285–1289. doi:10.1111/j.1524-4725.2005.31204
37. Kassir R, Kolluru A, Kassir M. Intense pulsed light for the treatment of Rosacea and Telangiectasias. J Cosmet Laser Ther. 2011;13(5):216–222. doi:10.3109/14764172.2011.613480
38. Ying C, Xiufen Z, Hongfeng T, et al. Observation on the efficacy of intense pulsed light combined with multi-band in the treatment of moderate and severe acne. J Diagn Treat Skin Venereal Dis. 2015;22(05):361–365. doi:10.3969/j.issn.1674-8468.2015.05.003
39. Chalermsuwiwattanakan N, Rojhirunsakool S, Kamanamool N, Kanokrungsee S, Udompataikul M. The comparative study of efficacy between 1064‐nm long‐pulsed Nd:YAG laser and 595‐nm pulsed dye laser for the treatment of acne vulgaris. J Cosmet Dermatol. 2021;20(7):2108–2115. doi:10.1111/jocd.13832
40. Jasim ZF, Al-Qarqaz F, Handley JM. To the editor: effect of single pulsed dye laser treatment on acne vulgaris. Dermatol Surg. 2005;31(11):1483. doi:10.1097/00042728-200511000-00025
41. Cassuto DA, Ancona DM, Emanuelli G. Treatment of facial telangiectasias with a diode-pumped Nd:YAG laser at 532nm. J Cutan Laser Ther. 2000;2(3):141–146. doi:10.1080/14628830050516399
42. Soltes B. Intense pulsed light therapy. Obstet Gynecol Clin North Am. 2010;37(4):489–499. doi:10.1016/j.ogc.2010.09.005
43. Monib KME, Hussein MS. Nd: YAG laser vs IPL in inflammatory and noninflammatory acne lesion treatment. J Cosmet Dermatol. 2020;19(9):2325–2332. doi:10.1111/jocd.13278
44. Tanaka Y, Tsunemi Y, Kawashima M. Objective assessment of intensive targeted treatment for solar lentigines using intense pulsed light with wavelengths between 500 and 635 nm. Lasers Surg Med. 2016;48(1):30–35. doi:10.1002/lsm.22433
45. Lee Y, Jang JH, Nam S, et al. Investigation of prognostic factors for intense pulsed light treatment with a vascular filter in patients with moderate or severe meibomian gland dysfunction. J Clin Med. 2022;11(16):4724. doi:10.3390/jcm11164724
46. Elman M, Lask G. The role of pulsed light and heat energy (LHETM) in acne clearance. J Cosmet Laser Ther. 2004;6(2):91–95. doi:10.1080/14764170410035584
47. Kurwa K. The role of photodynamic therapy in dermatology. Clin Exp Dermatol. 1999;24(3):143–148. doi:10.1046/j.1365-2230.1999.00439.x
48. Vora GK, Gupta PK. Intense pulsed light therapy for the treatment of evaporative dry eye disease. Curr Opin Ophthalmol. 2015;26(4):314–318. doi:10.1097/ICU.0000000000000166
49. Hongcharu W, Taylor CR, Aghassi D, Suthamjariya K, Anderson RR, Chang Y. Topical ALA-photodynamic therapy for the treatment of acne vulgaris. J Invest Dermatol. 2000;115(2):183–192. doi:10.1046/j.1523-1747.2000.00046.x
50. Bhardwaj SS, Rohrer TE, Arndt K. Lasers and light therapy for acne vulgaris. Semin Cutan Med Surg. 2005;24(2):107–112. doi:10.1016/j.sder.2005.04.001
51. Iinuma S, Farshi S, Ortel B, Hasan T. A mechanistic study of cellular photodestruction with 5-aminolaevulinic acid-induced porphyrin. Br J Cancer. 1994;70(1):21–28. doi:10.1038/bjc.1994.244
IPL Narrow Spectrum and Broad Spectrum PAE therapy | CCID - Dove Medical Press
Read More




No comments:
Post a Comment